


What is spirometry?

Spirometry measures the amount of air you can breathe out from your lungs and how fast you can blow it out. You’ll be asked to take a very deep breath and blow out as fast as you can into a mouthpiece, until no more air comes out.
A spirometry test typically takes 10 to 20 minutes, but may be longer if it includes bronchodilator responsiveness testing.
Types of spirometer
There are various different spirometer devices, but they all measure the same thing.
Many GP surgeries now have small, portable spirometers.
Some spirometers are more sophisticated and can give more detailed results. These are used in a hospital or clinic.

What is bronchodilator responsiveness testing?
Bronchodilator responsiveness testing is done to see if your lung function gets better with medication, and if so, by how much. It’s sometimes called reversibility testing. In bronchodilator responsiveness testing, the spirometry test is done before and after you breathe in some medication.
What’s spirometry used for?
Spirometry can help tell if your breathing is affected by narrowed or inflamed airways. The results are useful in diagnosing lung conditions such as COPD and asthma. For some conditions, it can be used to grade how severe your condition is.
How should I prepare for a spirometry test?
You’ll be told if there are any particular things you need to do to prepare. You may need to stop taking bronchodilator medication before the test. You should also stop smoking for 24 hours beforehand, if you can.
On the day of your spirometry test, it’s a good idea to wear loose, comfortable clothing.
Am I fit to do the test?
Spirometry is usually safe, but there are some conditions where it may cause problems. Tell your health care professional if any of these apply to you:
- angina
- heart problems
- recent concussion
- uncontrolled high or low blood pressure
- pulmonary hypertension
- pulmonary embolism
- pneumothorax
- recent surgery on the brain, middle ear, sinuses, eyes, chest or abdomen
- late term pregnancy
- aneurysms
They will often have a checklist to ask you about these. If in doubt, talk to your health care professional.
What happens during the test?
You will be asked some questions before you start, to check you are medically fit to do the test. It is important to put as much effort into the test as you can, so the results are accurate.
You’ll be asked to sit comfortably and may have a clip put on your nose to make sure all the air goes into the mouthpiece. You will be shown how to blow into the spirometer before starting. You may be asked to blow 3 or more times into the spirometer, to check the readings are similar each time.
Normally, you will first be asked to breathe in deeply and out gently. Once your health care professional is happy with the results, you will move on to the next part of the test. You will have to breathe in again deeply, this time quite fast, and then breathe out as fast and as hard as you can until your lungs are empty.
Your health care professional may ask you to use your inhaler or other medication, wait 15–20 minutes and then repeat the test. For some drugs the wait may be 45 minutes between tests. This is called a bronchodilator responsiveness test or reversibility test and it’s done to see if the medication improves your breathing. If you use inhalers, you should bring them to your appointment.
Occasionally, people feel a little light-headed and dizzy following the test. This usually lasts only a few moments. Let the person performing the test know, to make sure that you have time to recover.
What will the results look like?
Spirometry usually measures:
- how much air you can blow out in a relaxed manner, like a gentle sigh out, until your lungs are completely empty. This is called your slow vital capacity or VC
- the amount of air you can blow out in one second. With healthy lungs and airways, you can normally blow out most of the air from your lungs in one second. This is called your forced expiratory volume in one second, or FEV1
- the total amount of air you can blow out in one complete breath after taking a deep breath in. You will be asked to blow out as hard and as fast as you can until your lungs are completely empty. This is called your forced vital capacity or FVC
Your health care professional will look at how much air you can blow out in the first second (FEV1) and compare this to the total amount (FVC). This will give a percentage of air you can blow out in the first second.
Your results will look different depending on the type of spirometer used. Normally, your health care professional will compare your measurements with the normal range of values. The curves drawn by the spirometer showing the pattern of airflow are also important to help understand your results.
Understanding spirometry and narrow airways
Think of a 5-lane motorway that has been reduced to 3 lanes due to roadworks. The traffic will take longer to travel through that stretch of motorway.
In the same way, if your airway is narrower than normal, it will take you longer to empty your lungs of air.
A spirometer records how much air you can breathe out in one second. That will be less if your airways are narrower than someone of your sex, age, height and ethnicity with healthy airways. It can also compare that result to how much air you breathed out, to measure how much your airways are blocked. In someone with healthy airways, at least 70% of the total air they breathe out would be breathed out in one second.
An example of a (normal) spirometry result for a hospital spirometer

These two graphs show:
- peak expiratory flow volume loop when breathing in and out
- volume / time.
The table below the graphs shows the normal range of values for
- forced expiratory volume (FEV1). That’s the volume of air breathed out in one second, measured in litres
- forced vital capacity (FVC). That’s the total volume of air breathed out in one breath, measured in litres
- vital capacity (VC). That’s the total volume of air you can breathe out when relaxed, measured in litres
- the percentage of air blown out in the first second. This is calculated by dividing your FEV1 by your VC and multiplying by 100. In normal, healthy lungs, this will be 70% or above.
If your best effort is below the minimum value (Min), your result is below what it is expected it to be. This information and the shape of the loop will help your health care professional understand your results.
Patterns on a spirometry reading
A spirometry reading usually shows one of three main patterns. These depend on how much air you can breathe out and what proportion you can get out in the first second.
- normal pattern
- obstructive pattern
- restrictive pattern
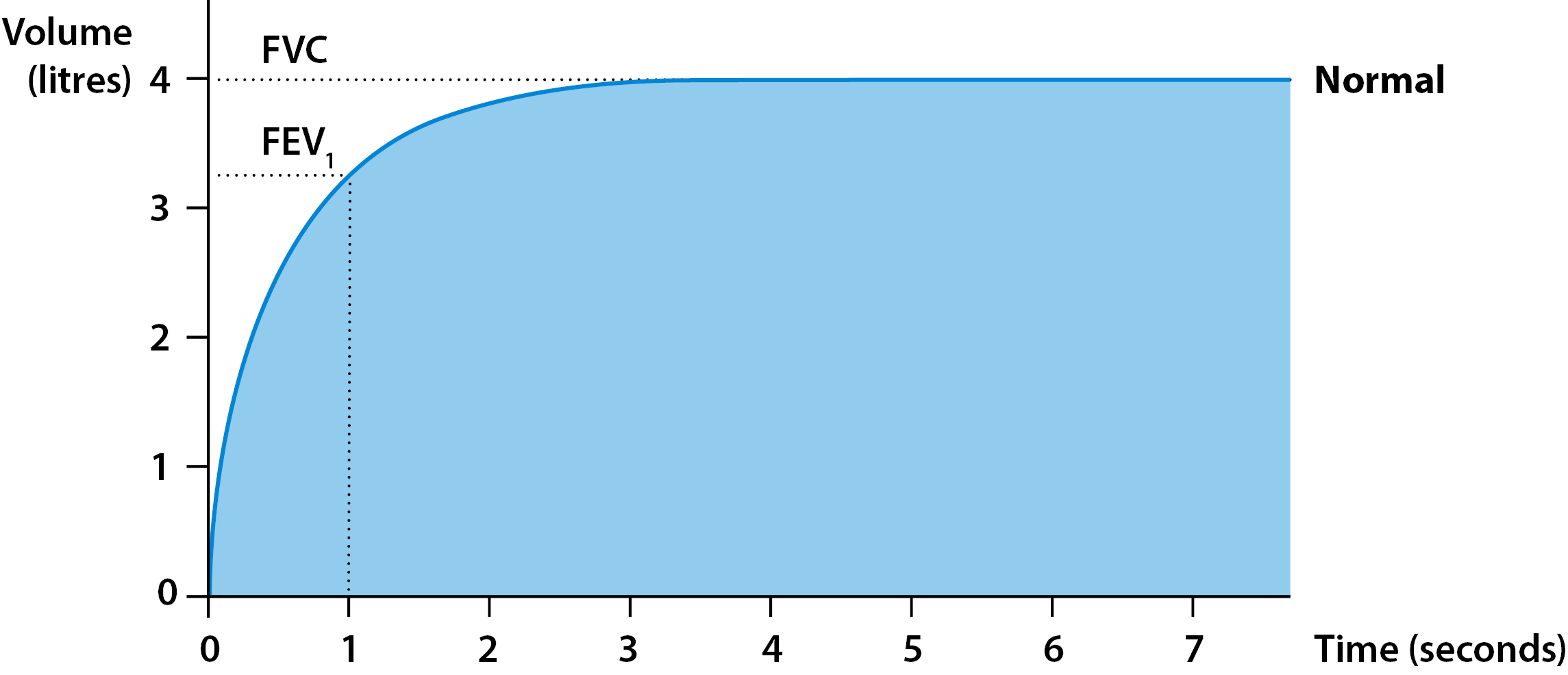
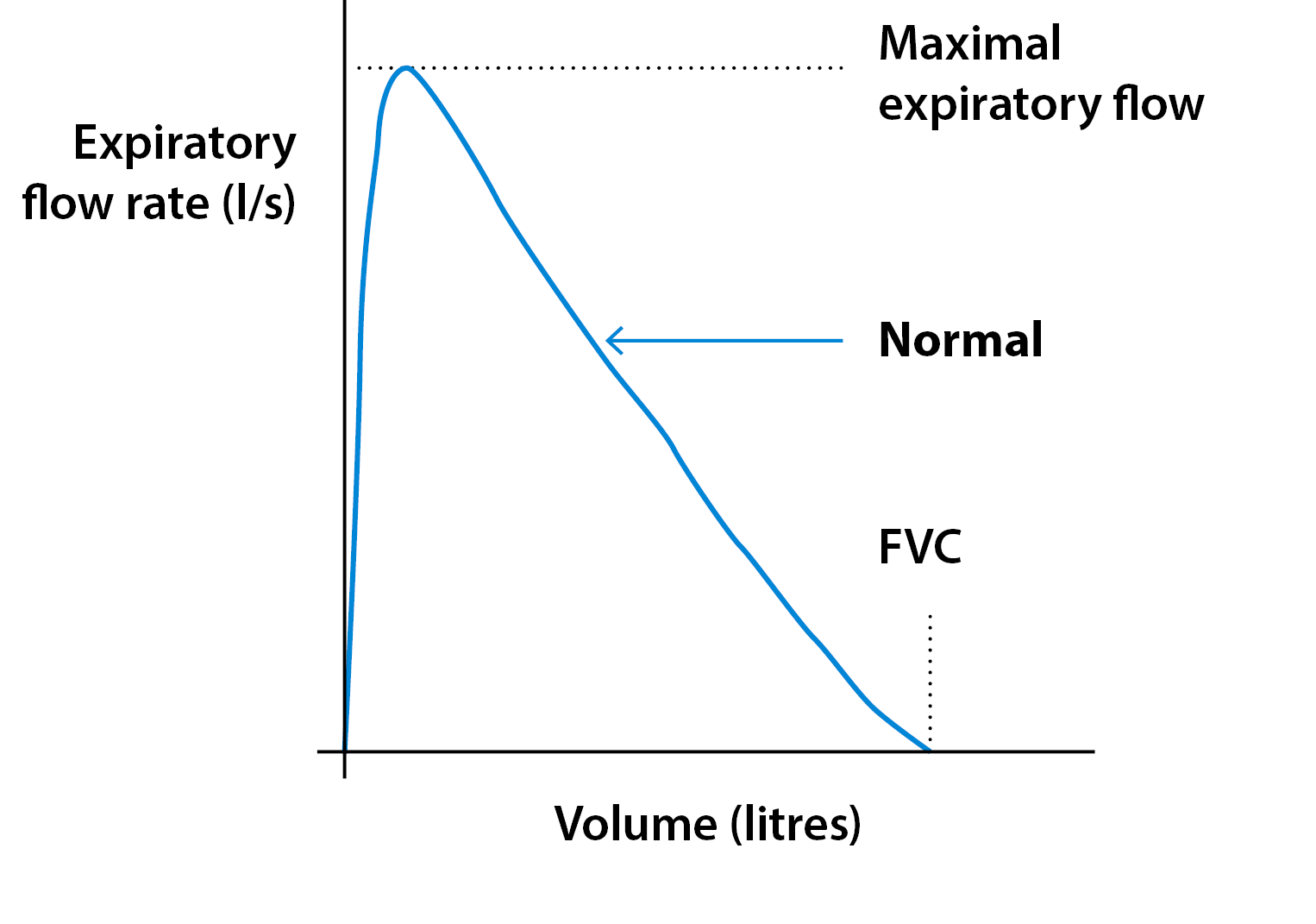
Normal pattern
Measuring FEV1 and FVC
Flow-volume measurement
Source: British Thoracic Society
The normal range is calculated by the spirometer based on your height, age, sex and ethnicity. If your lungs and airways are healthy, you can blow out most of your breath in the first second. This pattern tells your doctor that your spirometry test is normal when compared to the expected results for you.
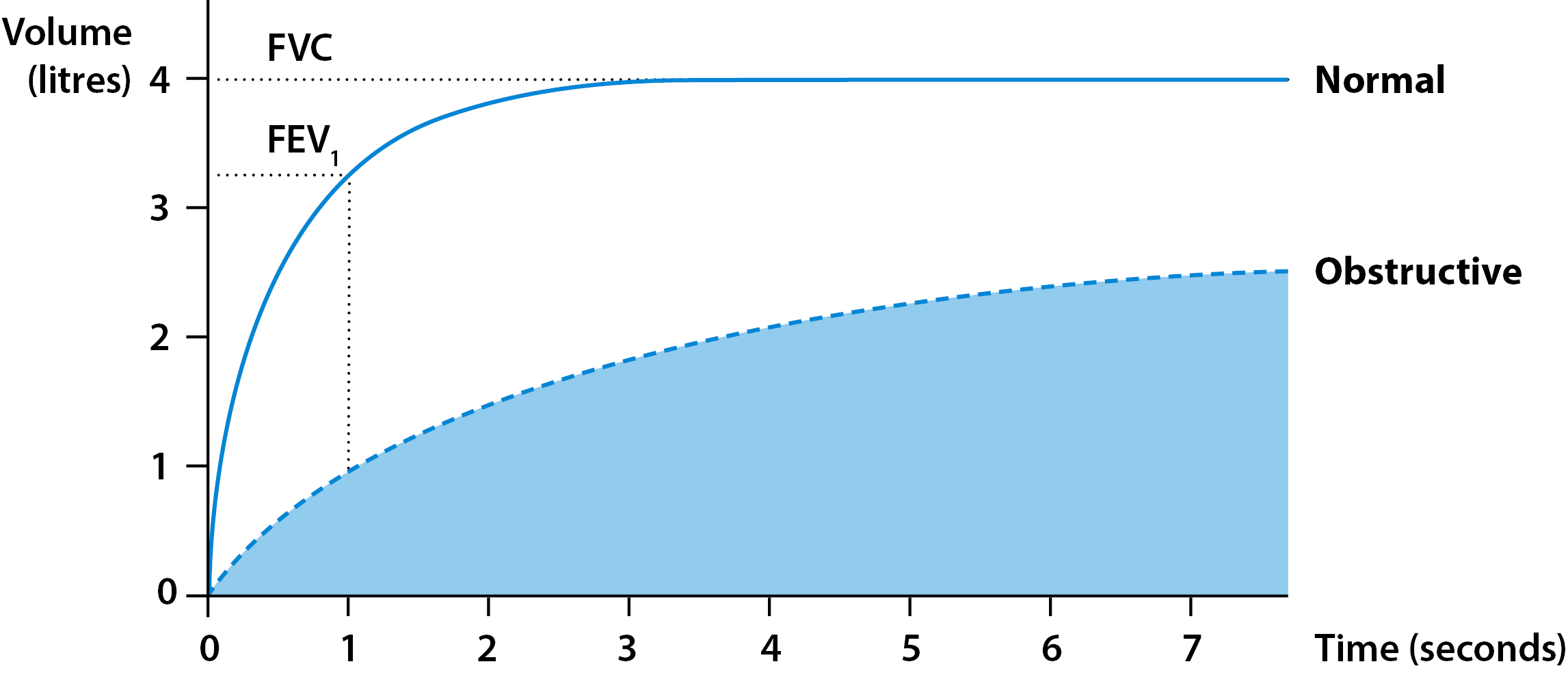
Obstructive pattern
Measuring FEV1 and FVC
Flow-volume measurement
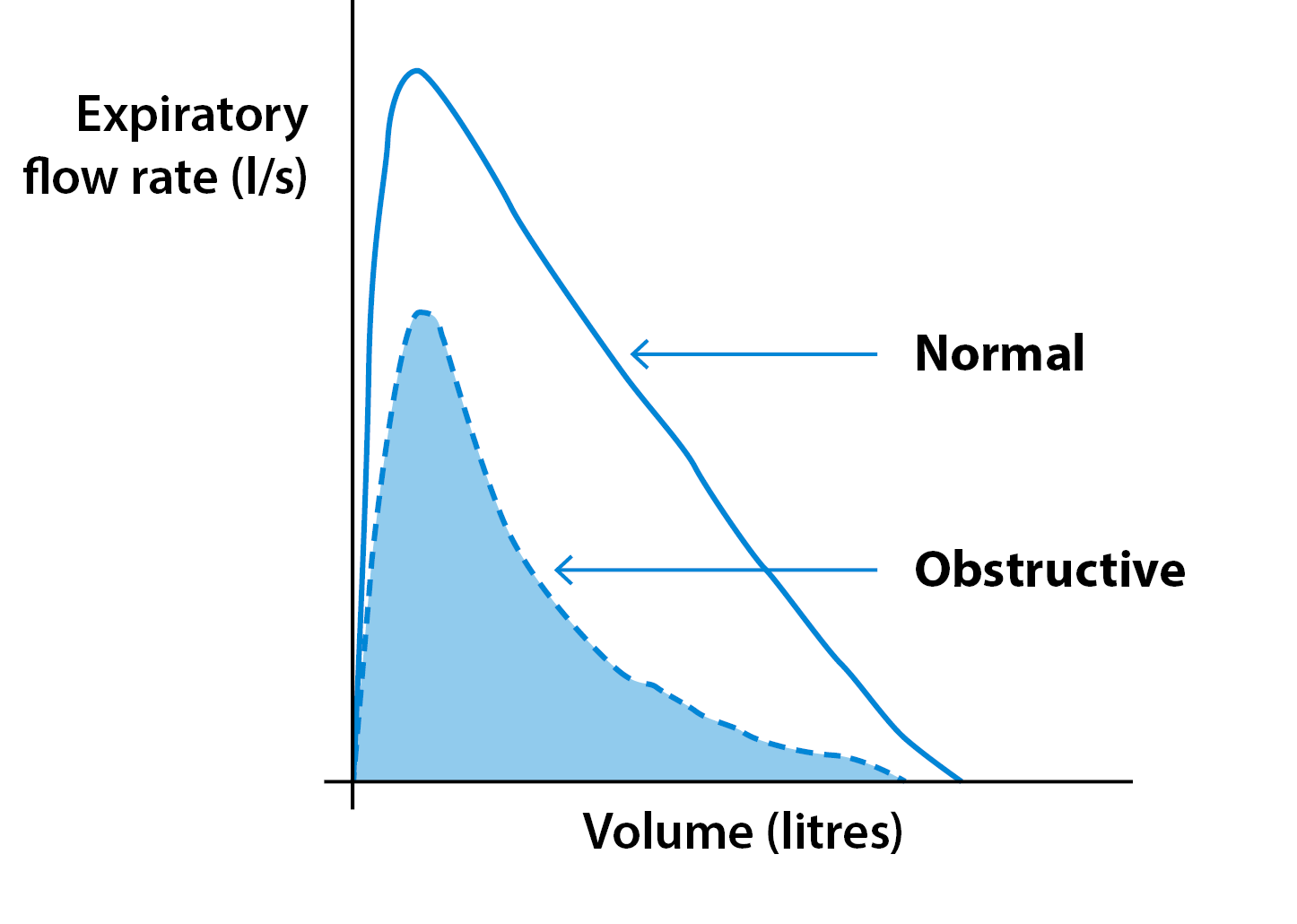
An obstructive pattern is typical if you have a lung condition that narrows your airways, such as COPD or asthma. This means that the air flows out of your lungs more slowly than it should (low FEV1) with less than 70% of the total amount in the first second.
Spirometry can help to assess if inhaled medication or inhalers can open up your airways by bronchodilator responsiveness testing (sometimes known as reversibility testing). Usually, medication causes a bigger change in scores if you have asthma than COPD.
People with COPD have an FEV1/FVC ratio lower than 70%. To decide how mild or severe your airflow obstruction is, the criteria below are used. It’s important to remember that people with the same degree of airflow obstruction may be more or less breathless than each other.
This is a guide:
| Grade of airflow obstruction | |
|---|---|
| Mild | FEV1 is 80% or more of the predicted value. If you have mild COPD, your spirometry test results can be normal after you take medication. |
| Moderate | FEV1 is 50-79% of the predicted value after medication |
| Severe | FEV1 is 30-49% of the predicted value after medication |
| Very severe | FEV1is below 30% of the predicted value after medication |
Source: NICE clinical guideline CG101: Chronic obstructive pulmonary disease in over 16s. June 2010, Table 4
Restrictive pattern
Measuring FEV1 and FVC

Flow-volume measurement:

With a restrictive pattern, the total amount of air you can breathe in is reduced but the speed you can breathe out is preserved. In this situation, both the FEV1 and FVC will be lower than predicted, but the ratio between the two will not be reduced.
A restrictive pattern can be caused by various conditions that affect
- the tissue of your lungs, or
- the capacity of your lungs to expand and hold a normal amount of air, such as pulmonary fibrosis.
If your results show a restrictive pattern, you may have a lung volume test to check if you have a low lung volume.
This pattern can also be seen in people who
- are significantly overweight
- have an abnormal curvature of the spine, or
- have weak breathing muscles.
Combined patterns
Some patients may have a combination of obstructive and restrictive patterns. This happens when both the total amount of air and how fast you can blow out are reduced. It happens in severe emphysema or cystic fibrosis, and can also happen if someone is obese.
We’re currently reviewing this information. An updated version will be available soon.